
When crisis meets the wrong environment
Imagine this.
You are in crisis. Not quietly struggling, but acutely unwell.
Someone calls 999 or drives you to the hospital. You arrive at A&E.
The lights are bright. The noise doesn’t stop.
A child is crying. Someone nearby is in visible pain.
There is nowhere quiet to sit, nowhere to breathe.
You wait. And wait.
For some people, this is the moment they decide not to come back, because the environment tells them they do not belong.
This is not a hypothetical. It is what has been happening across NHS A&Es for years. And it is, at least in part, what the government’s plan to build 85 co-located mental health emergency departments is intended to address.
I have been watching this policy develop closely. I have read the research, sat in the conversations with NHS CEOs, clinicians and facilities leads, and attended international conferences where healthcare systems further along this journey have shared what they’ve learned. And while I think the ambition behind this programme is right, I keep returning to a question being asked by NHS colleagues who are working with the £120m capital funding from government to build these:
What does a mental health emergency department actually look like?
The scale of what we’re trying to solve
The data from NHS emergency departments is significant. Between April 2024 and March 2025, mental health presentations made up around 2% of all A&E attendances. But because people with mental health complaints wait so much longer, they make up roughly 3% of the people in the department at any given moment. A disproportionate presence shaped by the environment’s inability to cater to their needs.
The nature of those presentations is also changing.
- Around 50% involve self-harm or suicidal behaviour.
- Another 34% involve hallucinations, distress, or complex behaviour.
These are high-acuity presentations. They require skilled, specialist assessment. Not a corner of a general A&E department staffed by people stretched across 100 other patients.
And yet here is the thing that stopped me when I read the Nuffield Trust’s recent analysis of this policy: if you removed mental health waits from A&E, overall waiting times would fall by about three minutes.
Just three minutes.
Which means these units are not, primarily, about fixing general A&E performance targets. They are about something more important, and more complex.
The people Mental Health A&Es could actually reach
The most compelling argument for mental health emergency departments is about the people in crisis who are not going to A&E (or other access points) at all to seek help.
A recent study found that around 77% of people who died by suicide had no record of an A&E attendance or hospital admission in the 30 days before their death. In other words, the majority of people in the most acute danger were not in the system at the moment when intervention might have been possible.
Zoë Billingham CBE, Chair of Norfolk and Suffolk NHS Foundation Trust, after visiting the Mental Health Crisis Assessment Service (MHCAS) at St Charles Hospital, CNWL:
A calm, welcoming, 24/7 service for people in crisis and presenting with serious mental illness
"No flashing lights, no long waits, no chaos. People can walk in directly, without a complex referral process, and are quickly assessed and treated by skilled psychiatrists, nurses, psychologists and peer support workers.”
The results: 371 admissions avoided, saving over 1,000 inpatient bed days • 677 fewer A&E attendances • Zero out-of-area placements
Source: LinkedIn post, Zoë Billingham CBE, 2025
Part of the reason is the environment. Patients have described typical A&E departments as “horrible” and “off-putting”. When someone is already overwhelmed and distressed, already afraid of what admission might mean, a noisy, chaotic waiting room full of strangers is not somewhere they will choose to go. Sometimes they will wait. And sometimes they will not.
A genuinely well-designed mental health emergency department, a safe haven, one that communicates safety rather than chaos, that is welcoming enough that people in distress might actually choose to attend could change that.
That is a more ambitious goal than clearing a waiting room. And it requires a different kind of design response.
The physical health problem nobody wants to unpick
Before we get to design, there is a clinical question that has to be addressed honestly.
Of all the people who attend A&E for mental health reasons, 42% are also flagged with a non-mental health diagnosis. Over 40% need some form of physical treatment, cardiac monitoring for overdose, intravenous fluids, medication administration or treating self-harm wounds. Mental and physical health emergencies are not two separate things, they arrive together.
The Nuffield Trust has noted that emerging mental health A&E services are handling this inconsistently. Some exclude patients with “urgent medical need.” Others include “psychological difficulties in the context of physical illness” but draw their own lines around what counts as too physically complex. These are more than policy decisions, they are design decisions. Where does the mental health unit end and the physical A&E begin? How close is close enough for safe escalation? How are clinical handovers managed for someone who is both psychotic and in need of medical attention?
The Royal College of Psychiatrists has been clear that co-location is essential precisely because of this complexity. The risk of fragmented care, missed comorbidities, and increased stigma all grow the further these units drift from acute physical services. But co-location is a location decision, not a design answer. It tells you roughly where to put the building. It says almost nothing about how the building needs to work.
What the international evidence can tell us
The UK is building something it has never built before. Other countries have been doing this for longer, and there is meaningful evidence available.
Earlier this year, at the ASHE PDC Summit in Houston, Texas, I attended a presentation by the team at CannonDesign, Stephanie Vito, Manjiri Bapat, and Aaron Hernon (Johns Hopkins Health System).
Who had been studying how the physical proximity of Behavioral Health Crisis Units (BHCUs) to emergency departments affects clinical outcomes across multiple international case studies. Their research defined four distinct proximity typologies, from directly adjacent to freestanding in the community, and tracked outcomes pertaining to ED wait times, length of stay from ED arrival to discharge, and inpatient admissions across each.
The findings are instructive, and more nuanced than a simple “closer is better” story. Freestanding units in community settings (Typology 4), furthest from the main ED, produced the greatest reductions in ED wait times, up to 98% in some settings, likely because they are most effective at diverting people entirely out of the emergency pathway. But units placed immediately adjacent to the ED (Typology 1) produced the strongest inpatient admission avoidance rates, up to 70%, keeping people stable in a step-down environment close to acute care. Units integrated with wider behavioural health services (Typology 3) showed the strongest reductions in overall length of stay, at up to 80%.
The CannonDesign team were careful to resist a reductive conclusion. Their finding was that distance from the ED is a variable, but not the only one. What shapes outcomes is the interaction between proximity, capacity, environment, model of care, and the continuum of services available downstream. The right answer depends on what the organisation is trying to achieve, and that requires clarity about goals before the building specification is written.
For the 85 units now being planned across the UK, that goal clarity is not yet in place.
The research also included detailed design and planning work for the Johns Hopkins Howard County Medical Center BHCU. The slides below illustrate what considered design for a crisis stabilisation unit can look like, from the spatial layout down to the feel of individual spaces.
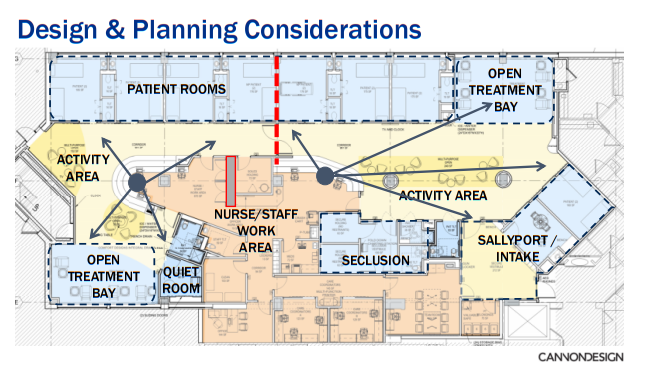
Overall floor plan: Johns Hopkins Howard County BHCU. Note the spatial separation of patient rooms, open treatment bay, activity areas, and staff work zone. Source: CannonDesign
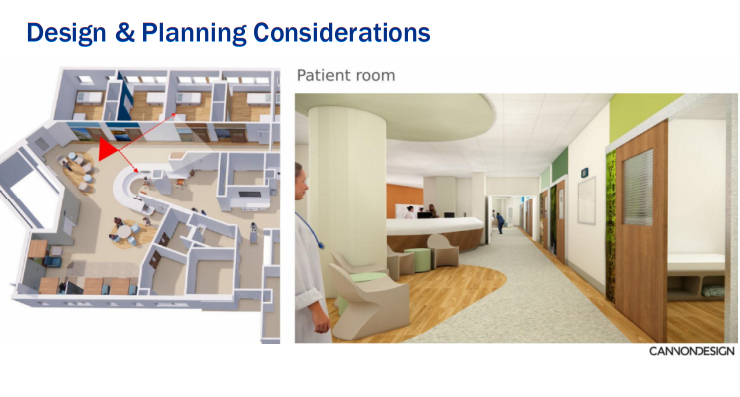
Patient room approach: soft lighting, wood tones, art, and visual privacy — a departure from the clinical aesthetic of general A&E. Source: CannonDesign
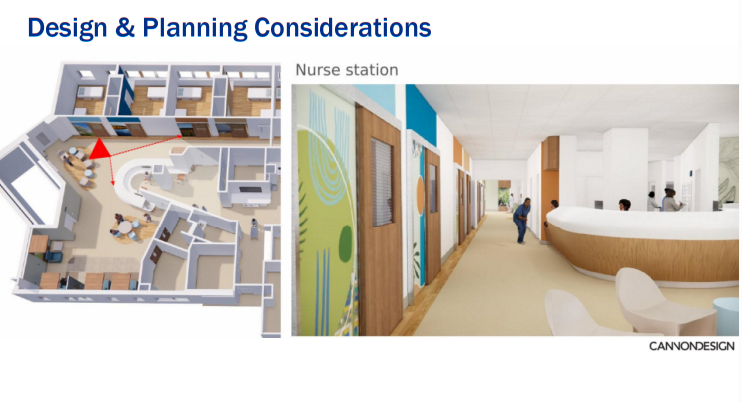
Nurse station: open sightlines, welcoming materiality, designed for calm oversight rather than surveillance. Source: CannonDesign
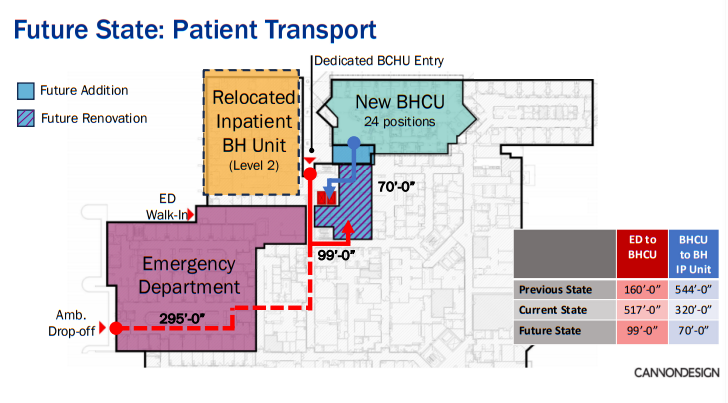
Future state planning at Johns Hopkins Howard County: the BHCU moves from 517’ to 99’ from the Emergency Department — illustrating how proximity decisions evolve as evidence builds. Source: CannonDesign
The question the brief hasn’t answered
Pilots are currently underway across 10 NHS trusts, and this is genuinely welcome.
And the sense of momentum is already being felt across the NHS, as highlighted in this recent LinkedIn post from a Mental Health Emergency Department National Learning Forum co-chaired by Jo Lomani and Modestas Kavaliauskas.
But speaking to the people responsible for delivering this programme - clinical leads, facilities directors, estates teams, a consistent picture emerges.
There is funding. There is policy direction. There is pressure to move quickly. What there is not, yet, is a design standard. In some cases, there also isn’t the revenue budget for staffing these new spaces.
Nobody has formally defined what a mental health emergency department needs to provide physically in the UK, what the environment should communicate to someone arriving in acute distress, what the spatial relationship between triage, assessment, and de-escalation spaces should be, what the lighting strategy should achieve, what access to outdoor space should look like, how the threshold between the mental health unit and the physical A&E should be navigated.
For example, what level of ligature reduction should we be delivering to? The risk profile of a mental health emergency unit, with higher acuity, greater clinical uncertainty, and a mixed population that has not yet been assessed, and is different from a mental health inpatient ward. The design response needs to reflect that difference, not simply copy what has been built for longer-term environments.
The pilots underway will generate learning. But the risk is that 85 buildings get specified and built before that learning is consolidated and shared, that we spend £120 million on units whose design brief was written too quickly, without enough reference to what already works internationally, and without enough co-production with the clinical teams and people with lived experience who will actually determine whether these spaces succeed. Then more is spent to solve problems at scale.
What good looks like, and what it needs
A mental health emergency department that is genuinely fit for purpose needs to hold several things at once.
It needs to be welcoming enough that someone who has been avoiding A&E for months might choose to come. It needs to be calm enough and approachable that someone in acute psychosis is not made more distressed by the environment. It needs clinical infrastructure close enough that someone with a suspected overdose can receive physical treatment without being transferred to another building, or worse, via a secure ambulance transfer. It needs de-escalation spaces that are genuinely de-escalating, not just quieter versions of the same hard environment. And it needs to be safe for both service users and staff.
None of these requirements are in conflict. But none of them can be designed by default. They require explicit decisions, made with input from clinical teams who understand the model of care, from people who know what it is to arrive in crisis, and from designers who have worked in this territory before.
The international evidence exists. The typology frameworks exist. The clinical guidance on what environments do and do not support recovery is more developed than the current UK policy process seems to recognise.
What is needed now is the will to slow down enough to apply it, before the concrete is poured.
A significant moment
I want to be clear about something. I think this programme matters. The idea that someone in acute mental health crisis should have access to an environment designed for their needs, staffed by people who understand those needs, built around a model of care that actually fits, is a condition of equitable care.
The 77% figure stays with me. Most of the people who died by suicide had no contact with emergency services in their final month. If even a fraction of that group might have attended a mental health emergency department because it felt safe and accessible, we could be saving hundreds, possible thousands of lives.
Getting this right requires honest engagement with the complexity. The design brief cannot be an afterthought. The model of care has to come first. The physical and mental health intersection has to be resolved, not deferred. And the voices of clinical teams and people with lived experience have to be in the room, they have the real knowledge of what put them off seeking help when they needed it.
At Safehinge Primera, we have been designing for mental health inpatient safety for years. We understand how the physical environment plays a key role as part of the clinical toolkit, how a door, a threshold, a corridor can shape the culture of a space more than any policy framework. If we can contribute to the conversation as the brief for these units is developed, we are here and ready to listen.
Contact the team discuss your Emergency Department plans.
Sources referenced
- Nuffield Trust / QualityWatch (January 2026): The changing terrain of mental health in A&E: specialised care or the same old bottlenecks? — Bea Taylor
- British Journal of Nursing (2025): A broken promise: the crisis of mental health care in emergency departments — Lindsey Udberg
- CannonDesign / ASHE PDC Summit (2026): Analyzing Behavioral Health Crisis Units’ Physical Proximity to EDs: Impact on Care — Manjiri Bapat, LEED AP BD+C, Stephanie Vito, AIA, ACHA, Aaron Hernon
- Royal College of Psychiatrists (2025): Response to NHS mental health A&E centre plans
- Centre for Mental Health (2025): Briefing 64 — Crisis and Acute Care
- Darzi Review (2024): Independent Investigation of the NHS in England
- NHS 10 Year Health Plan (2025)
- Zoë Billingham CBE (2025): LinkedIn post — Mental Health Crisis Assessment Service, CNWL






